Is South Africa our Preview of Global Case Trends?
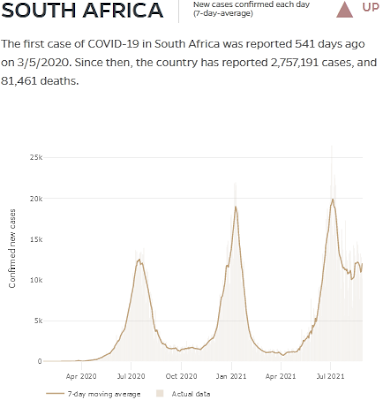
As SAGE implied in their 20th Technical Update's note 1.8.1 , we have effectively multiple serotypes of SARS-CoV-2 already, as Delta antisera doesn't neutralize B.1.351 nor B.1.621 virus meaningfully. That makes South Africa a potentially interesting case, because B.1.351 and C.1.2 emerged there. B.1.621 emerged in Colombia and has accounted for a significant percentage of cases, but Delta caused a serious wave in only South Africa. Beta was never recorded in Colombia and Delta barely touched them, and interestingly, they are now far below their record high infections, indicating that B.1.621 antisera is effective against its respective virus. https://origin-coronavirus.jhu.edu/region/colombia The lack of Delta's emergence could be geographic and political, but it may also mean that B.1.621 antisera is effective against Delta, which would be very encouraging news. https://outbreak.info/situation-reports?pango=B.1.621&selected=COL&loc=IND&loc=ZAF...